Proximal Hamstring tendinopathy
What are the Hamstrings?
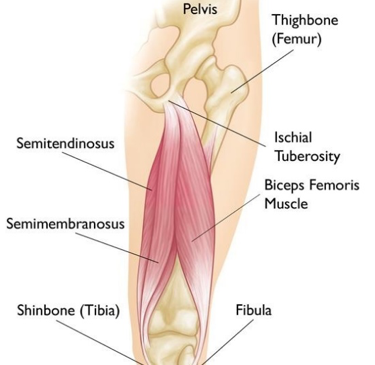
The hamstring muscle group comprises of 3 separate muscles; Biceps femoris (BF), Semitendinosus (ST) and Semimembranosus (SM). These muscles run down the back (posterior) of your thigh. With the exception of the BF short head, the hamstrings run from the ischium (bottom of your bum) at the pelvis down the back of the femur (thigh bone) and onto the tibia (shin) and fibula. These muscles together help produce both hip extension and knee flexion (bending the knee).
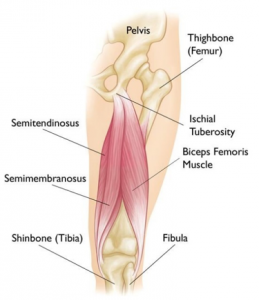
The Hamstring Muscles
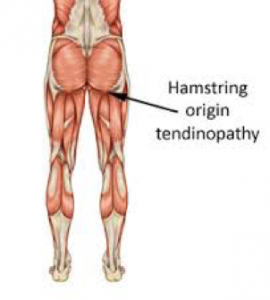
What is a Proximal Hamstring Tendinopathy?
Tendinopathy is a general term that describes the degeneration of a tendon and is normally a result of repetitive loading without sufficient recovery. Generally, it is a non-inflammatory injury that can become debilitating if not managed appropriately (Beatty et al, 2017 , Almekinders & Weinhold, 2015).
 They are commonly found in middle to long distance runners and regular gym goers who participate in movements such as; squats, lunges and change in direction running (Beatty et al, 2017 & Alfredson, 2014). Hamstring tendinopathies are worsened in prolonged sitting and standing due to the constant load.
They are commonly found in middle to long distance runners and regular gym goers who participate in movements such as; squats, lunges and change in direction running (Beatty et al, 2017 & Alfredson, 2014). Hamstring tendinopathies are worsened in prolonged sitting and standing due to the constant load.
What are the symptoms?
Proximal hamstring tendinopathies are being more recognized as a causative factor of sitting and activity related posterior hip pain. Unlike an acute tear you are more likely to experience;
- Gradual onset and increase in pain on tendon site
- Worsening pain PM and increased stiffness AM
- Tenderness on palpation
- Redness, increased temperature and swelling at location of tendon
(Ahmad et al, 2013)
Rehabilitation
Hamstring tendinopathies in their chronic form are able to get better when there is appropriate advice given from a professional Sports Therapist, GP or Physiotherapist.
Recent Comments